For medical weight-loss, wellness, MedSpa, metabolic-health, and primary care practices prescribing GLP-1 receptor agonists.
GLP-1 therapy has scaled faster than the cardiac protocols around it
GLP-1 receptor agonists — semaglutide, tirzepatide, liraglutide — have moved from diabetes to mainstream weight-management therapy. Medical weight-loss clinics, MedSpas with medical oversight, primary care, wellness practices, and metabolic-health programs are all prescribing them at unprecedented volume.
The therapeutic story is positive on the cardiovascular side at the population level: trials show meaningful reductions in major adverse cardiovascular events in eligible populations. But the individual-patient cardiac monitoring side has not kept up. Patients lose substantial weight quickly, change electrolyte balance, change autonomic tone, and sometimes change their medication burden — all conditions that warrant baseline and follow-up cardiac assessment.
A practical, in-clinic 12-lead ECG belongs in your GLP-1 protocol.
Cardiac considerations during GLP-1 therapy
The clinically relevant cardiac issues during GLP-1 therapy are not exotic; they are the predictable consequences of rapid weight loss combined with the known pharmacology of these agents:
- Resting heart rate increase. GLP-1 RAs are associated with modest sustained heart-rate increases (typically 2–4 bpm). Clinically meaningful in some patients with baseline tachyarrhythmia or autonomic dysfunction.
- Dehydration and volume contraction. Reduced oral intake, nausea, and occasional vomiting can shift volume and electrolyte status — with rate, rhythm, and QT consequences.
- Hypokalemia and hypomagnesemia. Plausible with prolonged reduced intake; both prolong QT.
- Medication interactions. Patients on QT-prolonging antiemetics (ondansetron), antidepressants, antibiotics (azithromycin), or antifungals deserve baseline QT documentation.
- Pre-existing arrhythmia. AFib, frequent ectopy, conduction disease — a baseline tracing is the difference between an informed conversation and a guess if symptoms emerge.
- Gastroparesis-related events. Rare but reported; clinical decision-making benefits from prior cardiac documentation.
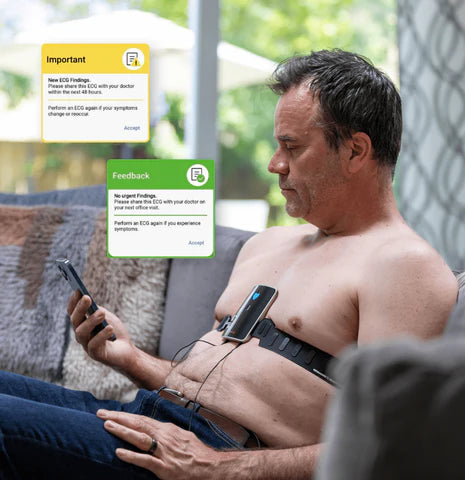
- Patient-reported palpitations. Common during early titration; a same-visit 12-lead ECG resolves them efficiently.

A practical baseline and follow-up cardiac protocol
A defensible, practice-friendly cadence:
- Baseline 12-lead ECG at the qualifying visit, before the first GLP-1 dose. Documents rhythm, rate, axis, intervals (especially QTc), structural clues, and any pre-existing findings.
- Follow-up 12-lead ECG at 12 weeks if any of: known cardiac history, baseline QTc > 450 ms, concomitant QT-prolonging medications, reported palpitations, or significant weight loss with electrolyte concerns.
- On-demand 12-lead ECG at any visit where the patient reports palpitations, lightheadedness, syncope, dyspnea, or chest discomfort.
- Annual 12-lead ECG for patients continuing GLP-1 therapy long-term, integrated with annual labs.
This protocol is conservative enough to be defensible and pragmatic enough to actually run inside a busy weight-loss or wellness clinic.
Why in-clinic 12-lead beats outsourced labs for this population
Outsourcing the 12-lead ECG to an external lab tends to fail in the weight-loss and wellness setting in four predictable ways:
- Drop-off. Patients don’t go. The baseline never happens, the protocol breaks.
- Timing. Results trail the visit by days or weeks, so the prescribing decision is made without the tracing.
- Fragmentation. The result lives in another system, not in your chart.
- Patient experience. Sending a cash-pay weight-loss patient to an outside lab for an ECG feels disjointed and reduces program retention.
An in-clinic portable 12-lead EKG eliminates all four failure modes.

The in-room workflow
A clean implementation looks like:
- Intake confirms history, current medications, baseline symptoms.
- Vitals captured.
- Portable 12-lead EKG performed by trained clinical staff in under a minute.
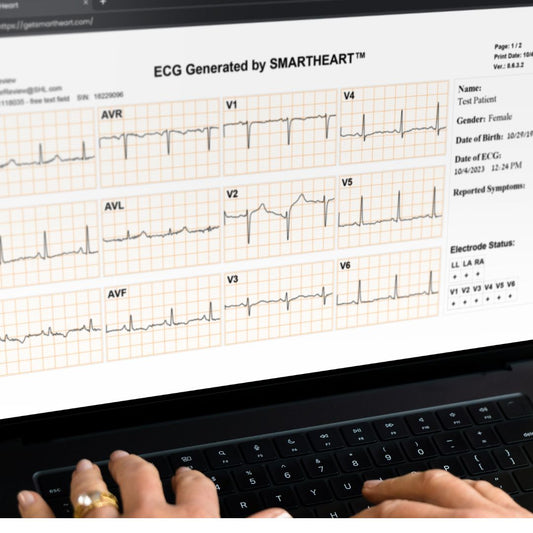
- Clinician interprets the tracing in real time on the paired tablet or phone; PDF saved to the chart.
- Findings reviewed with the patient as part of the GLP-1 consent conversation.
- Tracing available for comparison at the 12-week follow-up.
Documentation and program quality
- Baseline and follow-up tracings stored in the patient chart with timestamp and clinician signature.
- Documented interpretation and report supporting CPT 93000 family billing where applicable.
- HIPAA-compliant cloud storage with role-based access; tracings reviewable across the care team.
- Quarterly program review of baseline ECG completion rate as a quality metric.
Where SmartHeart fits
SmartHeart is an FDA-cleared, smartphone-paired portable 12-lead EKG built for practice-based clinical use, including medical weight-loss, wellness, MedSpa, and metabolic-health programs. It captures a clinical-grade 12-lead tracing in under a minute, stores recordings securely in the cloud, and is operable by any trained clinical staff member — a natural fit for the streamlined visit workflow these programs run.
Frequently asked questions
Are GLP-1 therapies cardiac-safe?
At the population level, GLP-1 RAs show favorable cardiovascular outcomes in eligible populations. Individual patients still benefit from baseline and follow-up cardiac documentation, particularly when on QT-prolonging co-medications or with prior cardiac history.
Do GLP-1 medications prolong the QT interval directly?
Current evidence does not establish direct QT prolongation as a class effect. Indirect risk through dehydration, electrolyte changes, and concomitant medications is the practical clinical concern.
Is an ECG required to prescribe semaglutide or tirzepatide?
It is not a regulatory requirement. It is a practice-quality decision. Programs integrating baseline and follow-up ECG strengthen their safety profile and patient experience.
Can a wellness or weight-loss clinic bill CPT 93000?
Yes, when a clinically valid 12-lead recording is captured and the clinician documents an interpretation and report. Coverage and reimbursement depend on the payer mix and program model (insurance, cash-pay, employer).
Add baseline and follow-up 12-lead ECG to your GLP-1 protocol
If your medical weight-loss, wellness, MedSpa, or metabolic-health practice is operationalizing GLP-1 protocols and wants integrated cardiac monitoring, SmartHeart’s clinical team can map the workflow to your setting.
Learn more about SmartHeart for Healthcare Professionals →
SmartHeart is intended for use by trained healthcare professionals in clinical and practice-based settings. Clinical interpretation of ECG recordings is the responsibility of a licensed clinician. SmartHeart is FDA-cleared for 12-lead electrocardiogram recording. This article is general information for clinicians and not a substitute for the clinician’s judgment in an individual patient’s care.