For primary care, urgent care, home health, and any clinician who sees patients before cardiology does.
The AFib detection gap in outpatient care
Atrial fibrillation is the most common sustained arrhythmia in adults, affecting an estimated 1 in 11 people over the age of 65. It is also one of the most consequential: undiagnosed AFib carries a 5-fold increase in stroke risk. Yet a large share of incident AFib is first identified not in cardiology but in primary care, urgent care, and home health — the exact settings that historically have not had reliable in-office 12-lead ECG capability.
The result is a quiet diagnostic gap. A patient mentions intermittent palpitations or fatigue. The clinician palpates an irregular pulse. The conversation that follows is usually some version of: “I think this might be AFib. We need to get an ECG.” If that ECG can’t happen in the room, the workup fragments — outside lab, cardiology referral, repeat visits — and AFib detection slips.
A portable 12-lead EKG closes that gap. A clinical-grade 12-lead tracing, captured in under a minute by any trained staff member, turns AFib detection into a same-visit decision.
What is atrial fibrillation, clinically?
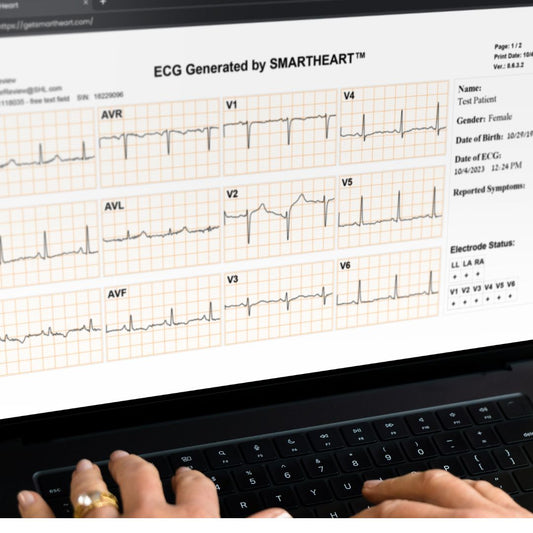
AFib is a supraventricular arrhythmia characterized by uncoordinated atrial activation, leading to ineffective atrial contraction and an irregularly irregular ventricular response. On a 12-lead ECG, the diagnostic fingerprint is:
- Irregularly irregular R-R intervals
- Absence of distinct P waves
- Fibrillatory baseline (most visible in lead V1)
Heart rate in untreated AFib typically runs 110–160 bpm but can be normal in rate-controlled or paroxysmal AFib. Rhythm strips alone can suggest AFib; a 12-lead ECG confirms it and screens for the structural and ischemic clues that change the management plan (left atrial enlargement, LVH, prior MI, pre-excitation, QT prolongation from rate-control medications).

Common AFib symptoms patients describe
AFib is heterogeneous. The classic presentation is palpitations, but a meaningful fraction of patients are asymptomatic and present only with a complication. Symptoms HCPs should not underweight:
- Palpitations — often described as “fluttering,” “racing,” or “thumping”
- Fatigue or reduced exercise tolerance
- Dyspnea on exertion
- Lightheadedness or near-syncope
- Chest discomfort (rate-related)
- New onset of stroke or TIA — sometimes the first presentation
In many outpatient practices, the trigger that finally produces a 12-lead ECG is a smartwatch alert, a routine vital with an irregular pulse, or a casual mention of palpitations on history.
A practical AFib workup in the outpatient setting
The minimum diagnostic standard for new AFib is a 12-lead ECG showing AFib in the patient. A rhythm strip from a single-lead device can suggest AFib, but it is not sufficient on its own to start anticoagulation, schedule cardioversion, or rule out the structural findings that change management.
A streamlined outpatient AFib workflow looks like:
- History and exam (CHA₂DS₂-VASc and HAS-BLED in mind).
- In-office 12-lead ECG — ideally the same visit.
- Basic labs: TSH, CBC, BMP, magnesium.
- Echocardiogram (timing depends on stability and structural concerns).
- Risk-stratified decision on rate control, rhythm control, and anticoagulation.
Step 2 is where most clinics lose time. A portable 12-lead EKG turns that step from a deferred referral into a 60-second in-room test.

Why a portable 12-lead EKG beats deferring to cardiology
The argument for an in-office portable 12-lead EKG in AFib detection is not theoretical:
- Diagnostic confirmation when AFib is present — you don’t lose the rhythm during paroxysmal episodes.
- Anticoagulation timing — earlier confirmation supports earlier stroke risk mitigation.
- Faster referrals when needed — cardiology gets the tracing with the consult.
- Captured CPT 93000 — a legitimately reimbursable service in primary care.
- Reduced patient anxiety — “you had it, we have it on paper, here’s the plan” beats “come back next week.”
Beyond detection: what the 12-lead changes
Once AFib is confirmed, the same 12-lead recording guides several decisions a single-lead rhythm strip cannot:
- Rule out pre-excitation (WPW) before AV-nodal blockers.
- Screen for prior MI, LVH, or conduction disease that changes rate vs rhythm control strategy.
- Establish a baseline QTc before adding QT-prolonging antiarrhythmics.
- Identify atrial flutter or other supraventricular rhythms that mimic AFib clinically but are managed differently.
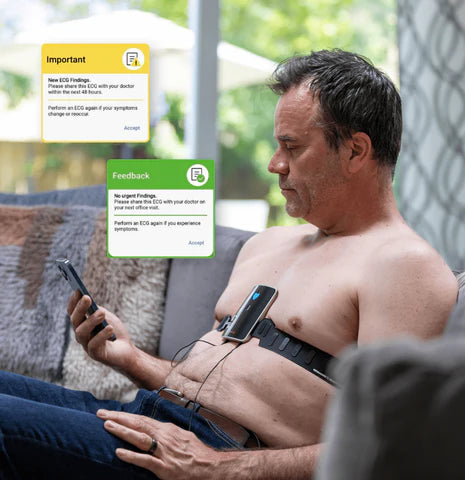
Where SmartHeart fits
SmartHeart is an FDA-cleared, smartphone-paired portable 12-lead EKG built for outpatient clinicians. It captures a clinical-grade 12-lead tracing in under a minute, stores recordings securely in the cloud, and is operable by any trained clinical staff member — no dedicated ECG technician, no cart, no paper. For AFib detection, that means the moment a patient mentions palpitations or you palpate an irregular pulse, you can confirm or rule out AFib in the same visit.
Frequently asked questions about AFib detection
Can a smartwatch reliably diagnose AFib?
Consumer single-lead devices and smartwatch ECGs can screen for AFib and are reasonable triggers for clinical workup, but they are not a diagnostic substitute for a 12-lead ECG read by a licensed clinician.
What if the patient is in AFib only sometimes?
Paroxysmal AFib often requires longer-duration monitoring (Holter, patch, or event monitor). A portable 12-lead EKG remains the standard for any episode caught in clinic and for the baseline recording that complements ambulatory monitoring.
Can I bill CPT 93000 for in-office AFib evaluation?
Yes, when a clinically valid 12-lead recording is captured and the clinician documents an interpretation and report. Confirm coverage rules with each payer.
Does the patient need to be in AFib at the time of capture for it to count?
To document AFib on a 12-lead ECG, yes — the rhythm must be present. For ongoing surveillance of paroxysmal AFib, longer-duration ambulatory monitoring is the better tool, paired with a baseline 12-lead in clinic.
Bring portable 12-lead EKG into your AFib workflow
If your practice is closing the AFib detection gap and exploring a portable 12-lead EKG or mobile EKG machine, SmartHeart’s clinical team can walk through workflow, integration, and reimbursement.
Learn more about SmartHeart for Healthcare Professionals →
SmartHeart is intended for use by trained healthcare professionals. Clinical interpretation of ECG recordings is the responsibility of a licensed clinician. SmartHeart is FDA-cleared for 12-lead electrocardiogram recording.