For primary care, urgent care, cardiology, and any outpatient clinician seeing more patients with wearable-triggered visits.
The wearable-triggered visit is now a standard outpatient pattern
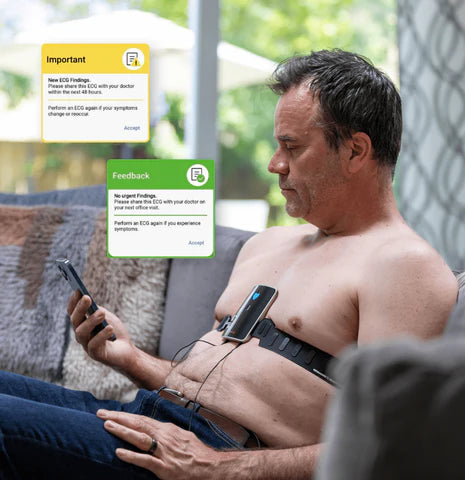
Apple Watch, Samsung Galaxy Watch, Fitbit, and several patch monitors deliver irregular rhythm notifications and single-lead ECG recordings directly to patients. The downstream effect on outpatient practice is real: patients arrive in clinic with a phone screen open, a notification they don’t fully understand, and a question that is almost always some version of “do I have something wrong with my heart?”
Clinicians need a consistent, calm, evidence-aligned approach to these visits. Done well, they catch real disease early (especially AFib) and reassure patients with normal hearts. Done poorly, they generate anxiety, low-value testing, and avoidable referrals.
What consumer wearables actually capture
- Photoplethysmography (PPG)-based irregular rhythm notifications. The watch sees pulse irregularity over time. It does not record an ECG; it triggers a prompt to record one or to seek care.
- Single-lead ECG recordings. When the user touches the device crown or sensor, a 30-second single-lead recording is captured (analogous to lead I).
- Six-lead recordings. Some smartphone-paired consumer devices add limb-lead views.
- Adhesive patch monitors (Zio, BodyGuardian, etc.). Ambulatory 2–3-lead recordings over 7–14 days; clinician-ordered, not direct-to-consumer in most workflows.
None of these is a 12-lead ECG. They are screening and self-monitoring tools that can prompt clinical evaluation — not substitute for it.
The first 60 seconds of the wearable-triggered visit
An efficient opening:
- Ask the patient to open the device app and show you the alert or recording.
- Confirm whether it is an irregular rhythm notification (PPG-based, no waveform) or an ECG recording (waveform present).
- For ECG recordings, look at: heart rate, regularity, P waves where visible, signal quality.
- Ask: was the patient symptomatic at the time of recording? At any other time?
- Ask: have they recorded multiple instances? Any in sinus rhythm?
That five-question opening directs the rest of the visit.

When to perform a clinical 12-lead EKG
A clinical 12-lead EKG is indicated in nearly all symptomatic wearable-triggered visits and in most asymptomatic ones when the alert is “possible AFib.” Practical triggers:
- Any current symptoms (palpitations, chest pain, dyspnea, syncope, lightheadedness).
- Single-lead device flagging “possible AFib.” A 12-lead is the appropriate confirmatory test.
- Irregular rhythm notifications recurring over time in a patient with cardiac risk factors.
- Pre-procedural patients whose wearable raised the question.
- Patients on QT-prolonging medications whose wearable raised concerns about rate or rhythm.
For asymptomatic, low-risk patients with a single unclassified or low-confidence recording, a clinician judgment call is appropriate. The downside of a 12-lead is low; the upside (catching real AFib, establishing a baseline) is meaningful.
How to counsel the patient
A useful script for the wearable-triggered visit:
“Your watch is a good screening tool. It noticed something that might be an irregular rhythm. It can’t make the diagnosis on its own — the next step is a proper 12-lead EKG so we can look at your heart from twelve different angles. Once we have that, we’ll know exactly what we’re dealing with and what to do next.”
Three things this does: validates the patient’s concern, sets realistic expectations about the wearable, and frames the 12-lead EKG as the clinical answer.

Wearable vs clinical ECG — side by side
Diagnostic scope
- Smartwatch/wearable: rhythm screening only.
- Clinical 12-lead EKG: rhythm, ischemia, axis, hypertrophy, intervals, conduction disease.
Operator
- Smartwatch: the patient.
- Clinical 12-lead: trained clinical staff member.
Clinical role
- Smartwatch: a screening prompt that should bring the patient to the clinician.
- Clinical 12-lead: the diagnostic test that informs management.
Documentation
- Smartwatch: patient-supplied data; reviewed and noted in the office visit.
- Clinical 12-lead: formal interpretation and report (CPT 93000 family).
Common pitfalls to avoid
- Treating a single-lead “possible AFib” as a confirmed diagnosis. Anticoagulation decisions warrant a 12-lead.
- Dismissing a wearable alert that is symptomatic. Even an “unclassified” recording in a symptomatic patient should prompt clinical workup.
- Skipping baseline structural assessment. The 12-lead doesn’t just confirm rhythm — it also screens for LVH, prior MI, pre-excitation, and QT findings that change management.
- Relying on the patient’s phone for the chart. The wearable recording can be a useful supplement, but the office 12-lead is the documented diagnostic study.
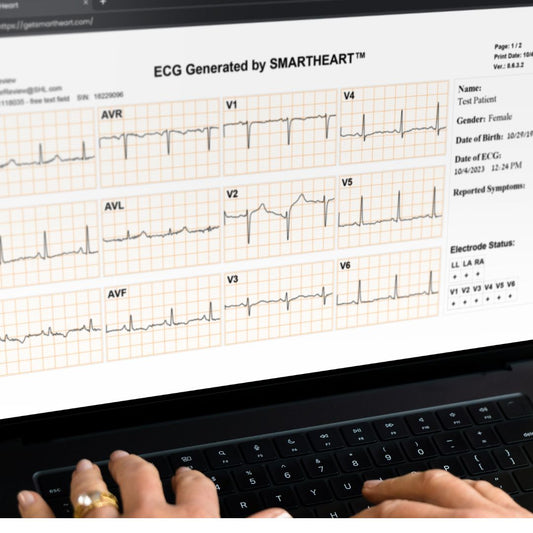
Where SmartHeart fits
SmartHeart is an FDA-cleared, smartphone-paired portable 12-lead EKG built for clinicians. It is purpose-designed to be the clinical follow-through for the wearable-triggered visit — a clinical-grade 12-lead tracing captured in under a minute by any trained clinical staff member, with secure cloud storage and easy sharing with cardiology.
Frequently asked questions
Is an Apple Watch ECG a real ECG?
Yes — it produces a real, single-lead ECG. It is not a complete diagnostic 12-lead ECG and should be treated as a screening prompt.
If a patient’s wearable says “normal,” do I still need to do an EKG?
It depends on symptoms, risk factors, and the clinical question. A “normal” single-lead recording does not rule out structural findings or paroxysmal arrhythmia outside the recording window.
Can I bill for reviewing a patient’s wearable recording?
Not as an in-office ECG. Review of patient-supplied data is captured in the office visit. A 12-lead ECG performed and interpreted in-clinic is a separate billable service (CPT 93000 family).
Are wearables a problem or a benefit for primary care?
On balance, a benefit. They identify a meaningful number of new AFib cases that would otherwise go undetected, and they prompt patients to seek evaluation earlier. The workflow tax is the additional visit volume — mitigated by an in-room 12-lead EKG that resolves the question the same day.
Make the wearable-triggered visit a same-day answer
If your practice is seeing more patients with smartwatch alerts and wants a streamlined 12-lead workflow for them, SmartHeart’s clinical team can map the workflow to your setting.
Learn more about SmartHeart for Healthcare Professionals →
SmartHeart is intended for use by trained healthcare professionals in clinical and practice-based settings. Clinical interpretation of ECG recordings is the responsibility of a licensed clinician. SmartHeart is FDA-cleared for 12-lead electrocardiogram recording. Product comparisons reflect publicly available device specifications.