For primary care, urgent care, home health, and any clinician deciding which cardiac test best answers the question in front of them.
Two tests, two very different questions
Holter monitors and portable 12-lead ECGs are often discussed together — both are “ECG” — but they answer different clinical questions. A 12-lead ECG is a high-resolution snapshot of the heart’s electrical activity right now. A Holter monitor is a lower-resolution movie of the heart’s rhythm over 24–48 hours.
Choosing the wrong one wastes time, money, and the patient’s trust. Choosing both — in the right order — is often the most useful path.
What is a Holter monitor?
A Holter monitor is an ambulatory ECG device that continuously records the patient’s rhythm for typically 24 or 48 hours (sometimes longer for extended Holters). It uses 2–3 leads, attached to the chest, with a small recorder worn on the body. The patient resumes normal activity while the device records every heartbeat.
Holter is the right tool when the clinical question is: “What is happening to this patient’s heart rhythm over time, especially during symptoms that don’t happen in clinic?”
What is a portable 12-lead ECG?
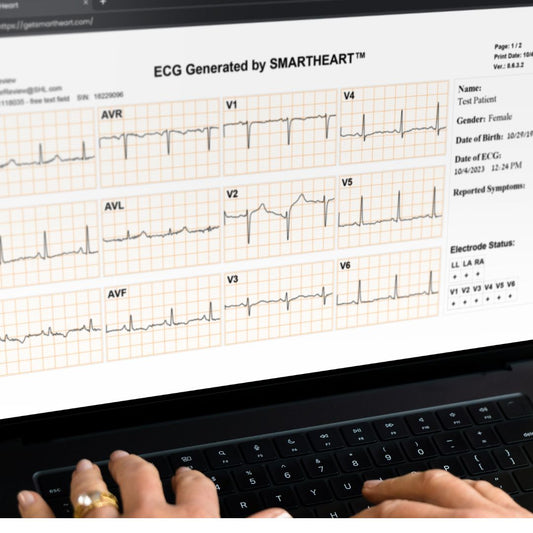
A portable 12-lead ECG (or 12-lead EKG) records the standard twelve simultaneous electrical views of the heart in a single 10-second tracing. Modern portable 12-lead devices are smartphone-paired, capture clinical-grade signal, and can be operated by any trained clinical staff member — no cart, no dedicated ECG technician.
Portable 12-lead is the right tool when the clinical question is: “What is the high-resolution electrical picture of this patient’s heart right now?”

Holter monitor vs portable 12-lead ECG — side by side
Duration of recording
- Holter: 24–48 hours (continuous).
- Portable 12-lead: 10 seconds (snapshot).
Leads captured
- Holter: typically 2–3 leads.
- Portable 12-lead: full 12 simultaneous leads (limb + precordial).
What it answers best
- Holter: intermittent rhythm questions — paroxysmal AFib, transient symptomatic palpitations, pause/bradycardia evaluation, AV-nodal disease.
- Portable 12-lead: structural and ischemic questions — ST-segment changes, axis, hypertrophy, bundle branch blocks, QT, pre-procedural clearance, confirming a rhythm in-clinic.
Workflow
- Holter: hookup, send patient home, retrieve device, upload, report — results often days later.
- Portable 12-lead: in-room capture in under a minute, results immediate.
Billing
- Holter: CPT 93224–93227 family (varies by services rendered).
- Portable 12-lead: CPT 93000 family (interpretation and report).
Patient experience
- Holter: wires, electrodes, and the device worn all day.
- Portable 12-lead: three minutes in the chair, no take-home equipment.
When to order which
Holter monitor when:
- Symptoms are intermittent and not present in clinic (palpitations, brief pre-syncope, transient bradycardia).
- You suspect paroxysmal AFib and need duration data.
- You’re assessing pause burden, PVC burden, or AV-block frequency.
- You’re titrating rate-control medications and need to see rates across daily activity.
Portable 12-lead ECG when:
- The patient is symptomatic now in clinic.
- You need to evaluate chest pain, ST-T changes, or possible ischemia.
- Pre-procedural or pre-operative clearance is required.
- You’re screening for LVH, conduction disease, or QT prolongation before starting a new medication.
- You’ve caught an irregular pulse on routine vitals and want to confirm AFib.

The combination that works best
In real outpatient practice, the most useful pattern is: portable 12-lead ECG first, Holter (or longer-duration patch) second if needed.
The 12-lead at presentation captures whatever the patient is in now, plus the structural baseline. If symptoms turn out to be intermittent and the 12-lead doesn’t catch them, a Holter or 14-day patch follows to find paroxysmal arrhythmia. Skipping the 12-lead and going straight to Holter is a common workflow mistake — it leaves a meaningful clinical gap.
Where modern patch monitors fit
Adhesive patch monitors (Zio, BodyGuardian, etc.) have largely replaced traditional Holter in many practices for durations beyond 48 hours. They are convenient, waterproof, and produce 7–14-day records. Patches answer the same intermittent rhythm questions as Holter; they do not replace a 12-lead ECG.
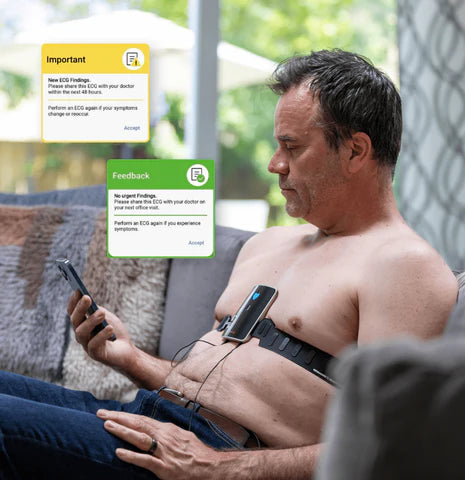
Where SmartHeart fits
SmartHeart is an FDA-cleared, smartphone-paired portable 12-lead EKG built for outpatient clinicians. It is purpose-designed for the in-clinic snapshot — the test that comes first in most palpitations, chest pain, and pre-procedure workflows — and is operable by any trained clinical staff member. Pair it with a patch or Holter for intermittent rhythm questions; use it on its own for everything else.
Frequently asked questions
Can a Holter monitor replace a 12-lead ECG?
No. A Holter records 2–3 leads over time. A 12-lead ECG records 12 simultaneous leads in a high-resolution snapshot. They answer different clinical questions.
Can a 12-lead ECG replace a Holter monitor?
Not for paroxysmal rhythm questions. A 12-lead ECG only captures what is happening at the moment of recording.
Is a patch monitor better than a Holter?
For durations longer than 48 hours, patch monitors are often preferred for patient comfort and adherence. For short rhythm questions, traditional Holter still works well.
What about smartwatches?
Smartwatch ECG features can screen for irregular rhythm but are not a diagnostic substitute for either a Holter or a 12-lead ECG.
Make the in-clinic 12-lead a same-visit capability
If your practice routinely defers 12-lead ECGs to outside labs or cardiology, SmartHeart’s portable 12-lead can bring that test back into the room — without a cart, a tech, or a paper trail.
Learn more about SmartHeart for Healthcare Professionals →
SmartHeart is intended for use by trained healthcare professionals. Clinical interpretation of ECG recordings is the responsibility of a licensed clinician. SmartHeart is FDA-cleared for 12-lead electrocardiogram recording.