For primary care, urgent care, home health, telehealth, and any clinician who orders an EKG test and needs to act on it the same day.
The EKG test, in one paragraph
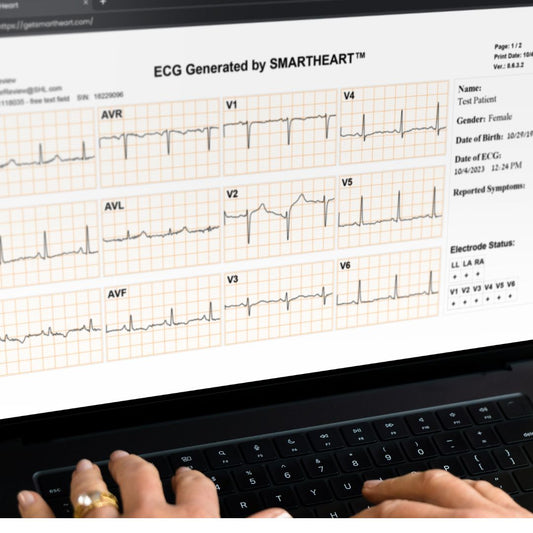
An EKG (electrocardiogram, also written ECG) is a non-invasive, 10-second recording of the heart’s electrical activity from twelve simultaneous leads. It is the highest-yield, lowest-cost cardiac test in outpatient medicine. The same recording answers rhythm, ischemia, axis, hypertrophy, conduction, and interval questions at once. When the test is ordered for the right reason and read with discipline, it changes management more often than any other simple in-office study.
When to order an EKG test in outpatient care
The practical indications cluster into five buckets:
- Symptoms suggesting cardiac etiology. Chest pain, dyspnea, palpitations, syncope or near-syncope, unexplained fatigue with exertional decrement.
- Suspected rhythm or conduction disorder. Irregularly irregular pulse, smartwatch alert, bradycardia, suspected AV block.
- Pre-procedural or pre-operative clearance. Sedation dentistry, ambulatory surgery, anesthesia screening, fitness-for-duty exams.
- Medication initiation or monitoring. Baseline QTc before QT-prolonging drugs; rate or rhythm control titration; psychotropic monitoring.
- Risk-based screening. Established cardiac history, diabetes with cardiovascular risk, hypertension follow-up, metabolic syndrome management, GLP-1 weight-loss programs.
EKG screening of asymptomatic, low-risk adults is generally not recommended by the USPSTF. The five buckets above describe clinically driven testing, not screening of the well.
Lead placement — the part that determines accuracy
Most diagnostic-quality issues with outpatient EKGs trace back to lead placement, not the device. The standard 12-lead arrangement:
- Limb leads (I, II, III + aVR, aVL, aVF): right arm, left arm, left leg, with right leg as ground.
- Precordial leads: V1 (4th ICS, right sternal border), V2 (4th ICS, left sternal border), V4 (5th ICS, midclavicular line), V3 (midway between V2 and V4), V5 (anterior axillary line, same horizontal as V4), V6 (midaxillary line, same horizontal as V4).
Common avoidable errors: V1/V2 placed too high (2nd or 3rd ICS) — produces a pseudo-incomplete RBBB and obscures anterior changes; limb leads swapped — produces axis chaos and bizarre P waves in lead I.

A disciplined reading sequence
A consistent reading sequence finds the high-yield findings reliably:
- Rate. Sinus, slow, fast, irregular.
- Rhythm. P before every QRS, QRS after every P, P axis, R–R regularity.
- Axis. Normal, left, right, extreme.
- Intervals. PR, QRS, QT/QTc.
- P wave morphology. Left atrial enlargement, right atrial enlargement.
- QRS morphology. LVH, RVH, bundle branch blocks, pathologic Q waves.
- ST segment. Elevation, depression, location, reciprocal changes.
- T waves. Inversions, hyperacute, low voltage.
- Comparison. Side by side with any prior tracing.
Common outpatient findings and what they trigger
- Normal sinus rhythm with no acute findings: document, reassure when symptoms are non-cardiac, continue planned workup if symptoms persist.
- AFib: CHA₂DS₂-VASc / HAS-BLED, rate or rhythm control discussion, anticoagulation decision, echo if not recent.
- Sinus tachycardia: identify cause (anxiety, fever, dehydration, hyperthyroidism, anemia, drug effect).
- PVCs/PACs: assess symptoms, frequency, structural concern.
- 1st-degree AV block: often incidental in healthy adults.
- LVH with strain: hypertension workup, echo, ambulatory blood pressure if appropriate.
- ST-T changes consistent with ischemia: escalate — ED for acute, cardiology curbside if subacute or atypical.
- Prolonged QTc: medication review, electrolytes, consider cardiology if persistent.
- Pre-excitation (WPW): cardiology referral; avoid AV-nodal blockers in AFib with pre-excitation.

When to escalate immediately
Patterns that should not be worked up in the office lane:
- Acute ST-segment elevation — STEMI activation.
- New-onset wide-complex tachycardia with instability.
- High-grade AV block with bradycardia and symptoms.
- Acute ischemic ST-depressions with chest pain and instability.
- QTc > 500 ms with concerning symptoms or contributing medications.
How a portable 12-lead EKG changes outpatient workflow
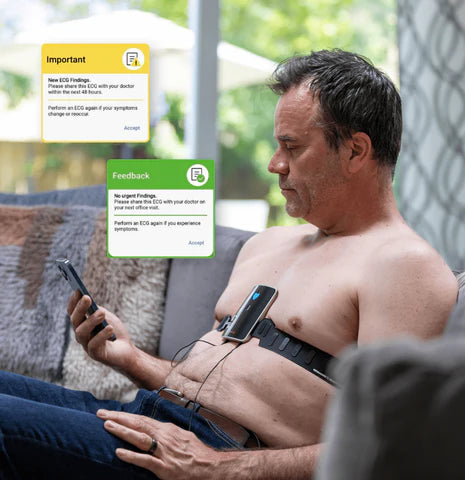
The biggest difference an in-room, portable 12-lead EKG makes is timing. The decision “does this patient need an EKG today?” is no longer a deferred lab order — it is a same-visit step. A clinical-grade tracing is captured in under a minute by any trained clinical staff member, reviewed in real time, and saved to the chart immediately. Borderline tracings can be shared with cardiology with the consult.
Where SmartHeart fits
SmartHeart is an FDA-cleared, smartphone-paired portable 12-lead EKG built for clinicians. It fits primary care, urgent care, home health, telehealth, occupational medicine, pre-procedural, and specialty workflows. It captures a clinical-grade 12-lead tracing in under a minute, stores recordings securely in the cloud, and is operable by any trained clinical staff member.
Frequently asked questions
How long does an EKG test take?
The recording itself is approximately 10 seconds. Setup (lead placement and patient positioning) typically adds 1–2 minutes with a portable 12-lead EKG.
What is the difference between an EKG and an ECG?
They are the same test. “EKG” derives from the German “Elektrokardiogramm.” “ECG” is the English abbreviation. Clinicians use them interchangeably.
Can I bill CPT 93000 in primary care?
Yes, when a clinically valid 12-lead recording is captured and the clinician documents an interpretation and report. Confirm coverage rules with each payer.
What if the patient is in AFib only intermittently?
The 12-lead remains the right test for any episode caught in clinic. Paroxysmal symptoms not present at the visit are best evaluated with ambulatory monitoring (Holter or patch).
Bring same-visit 12-lead EKG into your outpatient workflow
If your practice is operationalizing same-visit EKG testing, SmartHeart’s clinical team can walk through workflow, integration, and reimbursement.
Learn more about SmartHeart for Healthcare Professionals →
SmartHeart is intended for use by trained healthcare professionals in clinical and practice-based settings. Clinical interpretation of ECG recordings is the responsibility of a licensed clinician. SmartHeart is FDA-cleared for 12-lead electrocardiogram recording.