For primary care, urgent care, and any clinician who routinely hears “my heart was racing.”
The most common outpatient cardiac complaint
Palpitations are one of the highest-volume cardiac complaints in primary care and urgent care. Most palpitations are benign. A meaningful minority are atrial fibrillation (AFib) — the most common sustained arrhythmia in adults and the one with the largest preventable stroke burden. The clinical task is straightforward to state and hard to do well: distinguish benign palpitations from AFib in a single outpatient visit.
A 12-lead EKG captured during or immediately after the episode is the only test that fully answers the question. Anything else — history, exam, smartwatch alert, pulse palpation — is supporting evidence.
What does AFib feel like to a patient?
AFib symptoms cluster into patterns clinicians learn to recognize. The most common patient descriptions:
- “Fluttering” or “quivering” in the chest — the classic AFib palpitation.
- “My heart is racing and it’s not steady” — the irregularly irregular sensation.
- “It comes and goes for hours, then stops on its own” — paroxysmal AFib.
- Unexplained fatigue or reduced exercise tolerance — sometimes the only complaint.
- Mild lightheadedness or breathlessness on minor exertion.
Compare with benign palpitations, which patients more often describe as a single “skip” or “flip” — typical of PVCs or PACs — or a steady rapid heartbeat following caffeine, stress, alcohol, dehydration, or a missed meal (sinus tachycardia).
The outpatient differential for palpitations
The practical differential for new palpitations in an otherwise healthy adult:
- Sinus tachycardia — anxiety, dehydration, fever, anemia, hyperthyroidism, stimulants.
- Premature beats (PACs/PVCs) — the “skipped beat” sensation, usually benign in structurally normal hearts.
- Atrial fibrillation — irregularly irregular, often paroxysmal.
- Atrial flutter — regular at 150 bpm clue, sawtooth pattern in inferior leads.
- SVT — abrupt onset/offset, rates 150–220, narrow QRS.
- VT — wide-complex, hemodynamically significant; do not miss.
- Panic disorder — a diagnosis of exclusion in this setting.

History and exam clues that move you toward AFib
Higher-yield history points:
- Age over 60.
- Hypertension, diabetes, heart failure, prior stroke or TIA, sleep apnea, hyperthyroidism, alcohol use.
- Episodes lasting minutes to hours, often self-terminating, sometimes triggered by sleep loss or alcohol.
- Family history of AFib.
- Recent smartwatch alert flagging irregular rhythm.
Exam clues:
- Irregularly irregular pulse — the bedside sign that most reliably predicts AFib on ECG.
- Pulse deficit between auscultated apical rate and palpated radial rate.
- Signs of structural heart disease (S3, displaced PMI, mitral murmurs).
Red flags requiring escalation, not an office workup
Some presentations should not be worked up in an outpatient lane. Send to the ED:
- Hemodynamic instability (hypotension, altered mental status).
- Active ischemic chest pain.
- Syncope rather than near-syncope.
- Sustained wide-complex tachycardia.
- New onset of severe dyspnea or pulmonary edema.
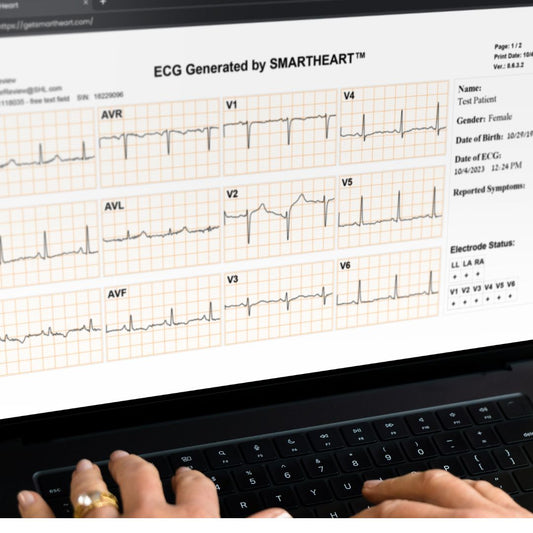
The same-visit 12-lead EKG decision
For everyone else, the highest-value test is a 12-lead EKG captured during the visit. A clinically valid 12-lead recording will tell you definitively whether the patient is in AFib at that moment, and — critically — also screens for the structural and ischemic clues that change management. A portable 12-lead EKG makes that test a routine in-room workflow rather than a referral.
When the 12-lead is normal during a current episode of “racing,” AFib at that moment is excluded; you can move on to PACs/PVCs, sinus tachycardia, anxiety, or longer ambulatory monitoring for paroxysmal arrhythmia. When the 12-lead shows AFib, anticoagulation and rate/rhythm decisions begin the same day.

What “AFib” actually means — in three sentences for patients
For patient counseling, a useful three-sentence explanation:
AFib is a common irregular heart rhythm that comes from the top chambers of the heart. It often feels like fluttering or racing, and many people don’t feel it at all. Untreated AFib raises stroke risk, which is why we want to confirm it on an EKG and decide together how to manage it.
Frequently asked questions
Can palpitations be normal?
Yes — most palpitations in structurally normal hearts are benign and related to PACs, PVCs, or sinus tachycardia. AFib is a meaningful minority; a 12-lead ECG during the episode reliably separates the two.
What causes AFib?
Risk factors include age, hypertension, sleep apnea, hyperthyroidism, alcohol, prior cardiac disease, and a family history. Some patients have no identifiable trigger.
Is a smartwatch enough to diagnose AFib?
Consumer single-lead devices and smartwatch ECGs are useful screening tools but are not a diagnostic substitute for a 12-lead ECG read by a licensed clinician.
If the 12-lead is normal, can I still have AFib?
Yes — paroxysmal AFib means episodes come and go. A normal 12-lead during a symptom-free moment does not rule out paroxysmal AFib; longer-duration ambulatory monitoring is the next step when clinical suspicion remains.
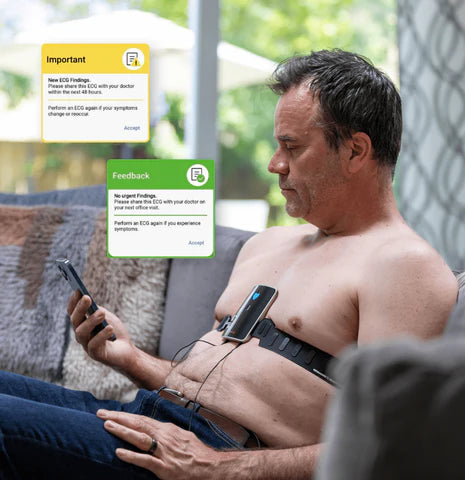
Bring same-visit 12-lead EKG into your palpitations workflow
If your practice wants to evaluate palpitations on the day they present, SmartHeart’s portable 12-lead EKG fits primary care, urgent care, home health, telehealth, and direct primary care workflows.
Learn more about SmartHeart for Healthcare Professionals →
SmartHeart is intended for use by trained healthcare professionals. Clinical interpretation of ECG recordings is the responsibility of a licensed clinician. SmartHeart is FDA-cleared for 12-lead electrocardiogram recording.