by Robert Beto M.D FACC
Acute Coronary Syndrome (ACS) represents a significant and urgent manifestation of coronary heart disease, which is responsible for a third of all deaths in individuals over the age of 35 in the United States. With its severe implications, ACS demands prompt and effective management to mitigate life-threatening complications and prevent recurrence.
Understanding Acute Coronary Syndrome (ACS)
Acute Coronary Syndrome encompasses conditions characterized by sudden, reduced blood flow to the heart, typically leading to a heart attack (myocardial infarction) or unstable angina. This umbrella term includes several clinical symptoms that correspond to acute myocardial ischemia. According to the American Heart Association, ACS affects over 1.4 million Americans annually, making it a leading cause of emergency medical care and hospitalization in the cardiovascular context.
Symptoms and Diagnosis of ACS
The onset of ACS can be dramatic and frightening, with symptoms including:
- Severe chest pain or discomfort, often described as a feeling of pressure, squeezing, fullness, or pain in the center of the chest.
- Pain or discomfort that spreads to the shoulders, arms, back, neck, or jaw.
- Shortness of breath.
- Sudden onset of sweating, nausea, or lightheadedness.
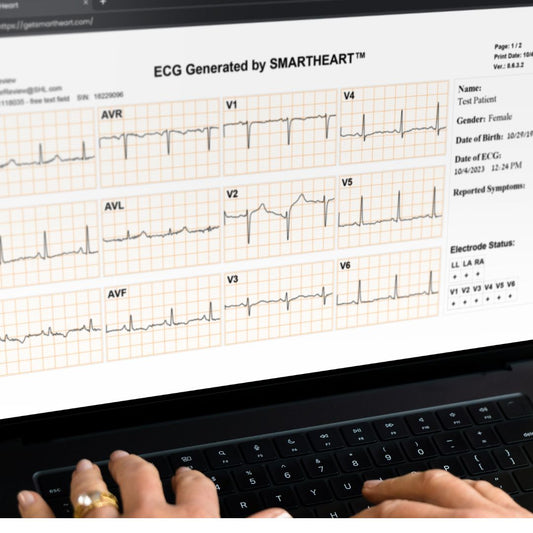
These symptoms require immediate medical evaluation, often involving an electrocardiogram (ECG) and blood tests to detect markers of heart damage. The prompt diagnosis is crucial for effective treatment and can significantly impact the prognosis.
Types of Acute Coronary Syndrome
ACS is classified into three types based on the severity and characteristics of the artery blockage:
- Unstable Angina (UA): Typically presents as new or worsening chest pain due to blood flow being intermittently disrupted in a coronary artery
- Non-ST-Segment Elevation Myocardial Infarction (NSTEMI): This is the next stage in the continuum from unstable angina. Here there is transient loss of blood flow in a coronary vessel leading to heart muscle necrosis or cell death. This is typically associated with extensively “blocked” vessels.
- ST-Segment Elevation Myocardial Infarction (STEMI): The pathophysiology here involves a mild to moderate plaque (non-occlusive) that becomes biologically active and ruptures. With the plaque rupture comes aggregates of platelets, red blood cells, and various cholesterol plaque particulates that suddenly occlude the coronary vessel.
Epidemiology and Risk Factors
ACS incidents are influenced by a variety of risk factors, including age, genetics, lifestyle choices, and existing health conditions such as hypertension, high cholesterol, diabetes, obesity, and smoking. Studies have shown that men are generally at a higher risk earlier in life compared to women, but the risk for women increases and may surpass that for men post-menopause.
Innovations in Post-ACS Management: Telemedicine and Portable ECGs
The traditional approach to managing ACS after initial treatment involves rigorous follow-up appointments and lifestyle management to prevent recurrence. However, the integration of telemedicine and portable ECG technology is revolutionizing this care paradigm. Telemedicine allows for continuous monitoring of patients' cardiovascular health from their homes or workplace thus enhancing convenience and compliance.
The Role of Portable ECG Devices
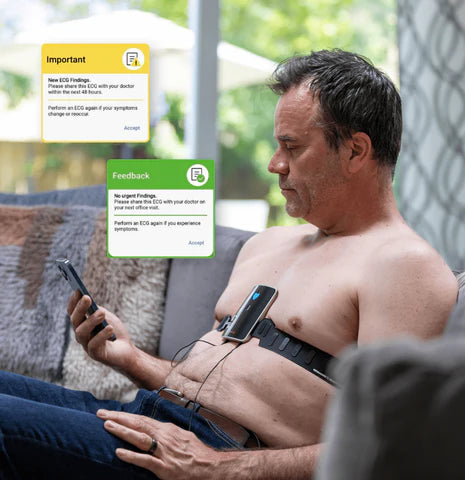
Portable ECG devices have become instrumental in the remote monitoring of patients diagnosed with ACS. These devices enable real-time tracking of heart rhythms and early detection of arrhythmias or ischemic changes, potentially preventing further acute episodes. The flexibility of portable ECGs facilitates more frequent assessments and adjustments to treatment plans based on nearly immediate feedback.
Exploring the TELE-ACS Trial: A Milestone in Cardiac Telemedicine
The TELE-ACS trial stands as a significant advancement in the management of Acute Coronary Syndrome, offering new insights into how telemedicine can enhance patient outcomes and revolutionize post-acute care strategies. This landmark study underscores the potential of integrating technology with traditional healthcare practices to optimize cardiac care.
Background and Objectives of the TELE-ACS Trial
Acute Coronary Syndrome, a severe manifestation of coronary artery disease, necessitates immediate and comprehensive management to prevent serious complications such as myocardial infarction and sudden cardiac death. Traditional ACS management often requires intensive follow-up and frequent hospital visits, placing substantial demands on both patients and healthcare systems.
The TELE-ACS trial was designed to assess whether a telemedicine-based approach could provide equivalent or superior care compared to the standard care protocol following an ACS event. The primary objectives of the trial included reducing hospital readmissions, minimizing emergency department visits, and improving patient satisfaction and overall cardiac health management.
Methodology of the TELE-ACS Trial
The trial enrolled participants who had recently experienced an ACS event. It divided them into two groups: one receiving standard post-discharge care and the other managed through a telemedicine approach. Participants in the telemedicine group were equipped with advanced remote monitoring tools, including the SmartHeart portable ECG device, a blood pressure monitor, and a pulse oximeter.
These patients regularly transmitted their health data to their care teams, allowing for real-time monitoring and early intervention. The care teams could adjust treatments promptly based on the data received, aiming to preempt any complications before they required hospitalization.
Key Findings and Impacts of the TELE-ACS Trial
The TELE-ACS trial demonstrated several significant benefits of using telemedicine in the management of ACS:
Reduction in Hospital Readmissions:
The telemedicine group saw a substantial reduction in hospital readmissions compared to the standard care group. This result not only indicates effective management but also suggests that remote monitoring can preempt the need for in-hospital care by addressing issues before they escalate.
Decrease in Emergency Department Visits:
Participants monitored through telemedicine reported fewer emergency visits, underscoring the efficacy of continuous, real-time health tracking in identifying and addressing potential problems early.
Improved Management of Cardiac Health:
The ongoing assessment provided by telemedicine allowed for timely adjustments in medication and lifestyle recommendations, which contributed to better overall management of patients' cardiac health.
Patient Empowerment and Satisfaction:
The trial noted high levels of patient satisfaction in the telemedicine group, largely due to the convenience, reassurance, and continuous support provided by remote monitoring. Patients felt more in control of their health, which is crucial for long-term condition management.
Cost-Effectiveness:
By reducing the need for physical follow-ups and unplanned emergency care, the telemedicine approach demonstrated potential cost savings for healthcare systems, making it a scalable option for widespread ACS management.
Future Implications
The success of the TELE-ACS trial paves the way for broader implementation of telemedicine in cardiac care, especially in managing chronic conditions like ACS where continuous monitoring post event can dramatically improve outcomes. The integration of such technology could redefine standard care practices, making healthcare more proactive, personalized, and patient-centered.
As the healthcare industry continues to evolve, the insights gained from the TELE-ACS trial will likely influence future policies, care protocols, and innovations in technology, further entrenching telemedicine as a cornerstone of modern cardiac care.
This elaboration on the TELE-ACS trial details its methodology, findings, and implications, providing a comprehensive view of its impact on the future of cardiac care management.
Conclusion
The TELE-ACS trial marks a pivotal advancement in the field of cardiology, demonstrating the transformative potential of telemedicine in managing Acute Coronary Syndrome. By significantly reducing hospital readmissions and emergency department visits, the trial not only showcases the effectiveness of remote monitoring systems but also highlights their role in enhancing patient outcomes and satisfaction. The success of the TELE-ACS trial suggests a promising future where telemedicine could become an integral part of post-ACS care, offering a more proactive, guideline driven, patient-centered approach.
This enhanced model of care not only optimizes health outcomes but also has the potential to alleviate the burden on healthcare systems by reducing the necessity for in-person visits and managing health resources more efficiently. As technology continues to evolve and integrate into healthcare practices, the insights from the TELE-ACS trial will likely guide future innovations and policies, shaping a new era in cardiac care that prioritizes accessibility, efficacy, and patient empowerment.
Incorporating the trial’s findings into broader clinical practices could lead to widespread adoption of similar telemedicine strategies across various aspects of healthcare, revolutionizing the way we approach chronic disease management and reinforcing the importance of adapting to technological advancements in medicine.
This conclusion reiterates the significant findings and broader implications of the TELE-ACS trial, aligning them with the overall theme of the blog and emphasizing the future possibilities in cardiac care.
Dr. Robert Beto is a cardiologist and CEO of HeartNexus'. He has extensive experience in managing acute coronary syndrome. With a commitment to leveraging technology for improved patient outcomes, Dr. Beto is dedicated to advancing cardiac care through innovative and effective solutions, including telehealth.
References
For more in-depth information and the latest research on ACS management, readers are encouraged to consult the Journal of the American College of Cardiology and resources provided by the American Heart Association. For detailed study results and further information on the TELE-ACS study published in the Journal of the American College of Cardiology, please click here.